Prosthodontics
Introduction to prosthodontics
Patient preparation before prosthetic phase
All-ceramic veneers and crowns
Complex prosthetic rehabilitation
Removable dentures, retention elements enhancing the stability of dentures
-
Introduction to prosthodontics
Dental prosthetic treatment is most often used to reconstruct the missing teeth. Another reason for prosthetic treatment is strengthening the existing tooth tissue, especially when the use of composite materials does not guarantee achieving durable, functional and aesthetic results. Finally, a third use of prosthodontics is to improve the aesthetics of patient's teeth by using crowns, veneers, or onlays.
Three Main Methods of Reconstructing Missing Teeth:
- Bridge, that is reconstruction based on patient's own teeth. Patients respond well to this type of treatment, and quickly adapt to the new conditions in their mouths. The prevailing opinion is that a bridge provides high comfort to the patient and the use of modern all-ceramic materials gives good aesthetic results.
Bridge can only be done if the patient’s tissues surrounding the abutment teeth are in good condition. The abutment teeth are teeth on which the crowns are based on.
Bridges cannot be done on teeth poorly anchored in the bone, teeth surrounded by unhealthy periodontium tissue, and finally, on teeth damaged by caries or mechanical trauma.
In dental prosthetics the most biologically valuable part of the tooth is the root. If the root is there and it is surrounded by healthy soft tissue and healthy bone, then the tooth can be rebuilt. It can be done with the help of milled or cast crown-root inlays or fibreglass inlays. Then the prosthetic crown can be placed, for example as bridge abutment. Without meeting the above conditions reconstructing the missing teeth with a bridge is impossible. Even the most expensive and the most advanced prosthetic work cannot compensate for the weakening of root tissues, deficiencies in bone or periodontium tissue surrounding the root.Adhesive bridges: in some cases, adhesive bridges can be made. In most patients, contouring grinding the abutment teeth is limited to a minimum, and in some cases it is not even necessary. We are talking here bridges based on additive veneers. However, indications for a permanent, rather than temporary adhesive bridge are quite rigorous. Not following the exact criteria may lead to loss of stability and detachment of the bridge from the patient's teeth.
If a fixed teeth reconstruction, e.g. bridge, is impossible or not recommended, the patient can be treated with removable dentures or prosthetic implant reconstruction. - Removable dentures are dentures which can be removed from the mouth. This is probably the oldest method of reconstructing the missing teeth. We distinguish between partial and complete dentures. Gum supported dentures are made of pink acrylic imitating gums, and artificial teeth embedded in the denture plate. Partial dentures have bent clasps made of steel wire. This type of dentures transfers the chewing force through the gum to the bone. The stability of dentures can be increased by using special paste or creams.
Dentures in which the acrylic plate is reinforced with a metal skeleton are called partial skeletal dentures. These are bonding dentures. The chewing force here is transmitted to the bone through gums and the patient's own teeth, on which the cast clasps rest. Stabilization in skeletal dentures is much better than with gum supported dentures. Patients also appreciate better aesthetics, durability and less discomfort during use.
Another type of dentures is dentures mounted to the remaining teeth or implants with the use of attachments. Here locks, bolts, magnets, latches, and beams are used. There is a variety of options depending on patient’s oral conditions and their expectations. - Dental implants: replacing missing teeth with implants is the newest method. This is a separate branch of dental prosthetics, described in detail in the Implantology section.
Veneers are the best way to improve the aesthetics of the anterior part of the dental arch. Veneers are usually done for aesthetic reasons, such as tooth discolouration, unsightly fillings, anatomical defects: congenital or acquired shape defects, or to change the spacing between the teeth (diastema and trema). Since the aesthetic aspect is very important here, the first step should be taking dental impressions and preparing diagnostic wax-up models. After the patient’s approval of the veneers’ shape, we can make a mock-up, where we choose the colour of the new teeth, and only then, after establishing the details we proceed with contouring grinding and taking impressions again. Veneers can be made of composites, but the best aesthetic results are achieved with porcelain. Veneers are cemented to teeth with composite cement.
- Bridge, that is reconstruction based on patient's own teeth. Patients respond well to this type of treatment, and quickly adapt to the new conditions in their mouths. The prevailing opinion is that a bridge provides high comfort to the patient and the use of modern all-ceramic materials gives good aesthetic results.
-
Patient preparation before prosthetic phase
Prosthodontics deals not only with reconstructing the missing teeth, but also with the aesthetic correction of the remaining teeth and with improving oral occlusion. Patients often think of the prosthetic phase as a key stage. We need to remember that prosthetic treatment often requires preparation treatment. Reconstructive procedures of prosthetic base tissue, periodontal treatment, orthodontic treatment, conservative treatment with endodontics are often the initial phase, which will only culminate in reconstruction of the missing teeth.
Significant atrophy of the alveolar bone in the vertical and buccal-palatal dimension. Without proper preparation of the prosthetic base, correct bridge placement is not possible. The patient complained of a strange shape of the teeth in the old bridge and retention of food over the span of the bridge. The treatment started with removing the old bridge and bone augmentation procedure. After the reconstruction of keratinized gums a new all-ceramic bridge was placed. Retention of food disappeared, there is no bleeding, and the patient has a nice tooth shape, which is important with high smile line. There are two more procedures planned: a bone regeneration surgery and a new all-ceramic bridge on the left side.



A similar situation, but this time in the mandible. Before the prosthetic phase it was advisable to prepare the prosthetic base first. In this case soft tissue microsurgery was enough to achieve satisfactory result.



The patient complained of swollen soft tissues adjacent to the bridge, retention of food, and bleeding gums. The three-year-old bridge was removed. The abutment tooth had extensive decay from the palatal side. There was also a significant loss of alveolar bone volume and lack of keratinizing gum under the bridge span. The missing alveolar tissue was rebuilt and after 3 months a new bridge was made. The results satisfy the patient.




We often encounter big discrepancies between the expectations of patients, who ask when their new teeth would arrive or when they would have a nice smile. Sometimes we also meet patients who attempt to control the treatment process, as per their awareness and expectations. It is a big challenge. Patients sometimes ask: "Please do not treat the root canals again. They don’t bother me. It doesn’t hurt at all." When there is a recommendation for tooth extraction (for example due to extensive destruction of hard tooth tissue, or lesions of the tissue surrounding the tooth), patients expect that hiding the tooth under the crown will solve the problem. Patients think that if the tooth is saved they will avoid extraction. Unfortunately, this is not proper treatment. It should be strongly emphasized that preparation treatment, including sometimes lengthy and laborious procedures is absolutely necessary.
Often there is a need for treatment on both jaws. The patient wanted to have a bridge placed in the mandible (upper jaw). He was not interested in prosthetic treatment in the mandible. He was not bothered with the lack of rear, side and lower teeth. Finally, the patient agreed to treat both jaws. Vertical dimension of occlusion was restored. Facial features have changed significantly.



Occasionally, patients with extensive number of teeth missing need temporary prosthetic work done, especially those patients with severe occlusion defects (the alignment of dental arches), and dental muscle and joint problems. Such procedure prolongs the whole treatment, increases the costs, but it is the only complete and correct therapeutic process in this case. Our bite is stabilized at the front by contacts of the upper and lower dental arch, and at the back by the temporomandibular joints. For each prosthetic solution where there is no stable position of dental arches against each other or there is lack of stable central relation, the use of a facebow is required. It is the only safe method of transferring the prosthetic plane of the upper dental arch relative to the base of the skull. This results in optimization of the position of dental arches relative to the temporomandibular joint, and the correct setting of mandible heads in condylar joints.
The patient complained of some problems with the temporomandibular joint. Previous prosthetic treatment was performed without aligning the occlusal plane. The old bridges were removed, endodontic treatment followed and the stumps of the abutment teeth were rebuilt. Then the clinical crowns of teeth 24 and 25 were elongated and keratinised gum was restored under the span of the lower bridge. The new bridges for upper and lower dental arch were made only in the last stage. A significant improvement was achieved, especially in the functioning of temporomandibular joint. The symptoms were alleviated.




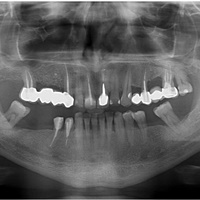
Preparing abutment teeth stumps plays an important role in prosthetic preparations. It may seem simple when we can limit to the reconstruction of supragingival part of the stump. When damage is also present below the gingival attachment, we have to deal with much more difficult situation.
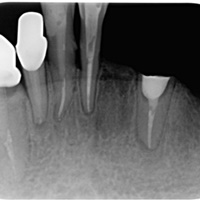
The following photos show a difficult periodontal case. In case of extraction of tooth 47, the patient will lose a chance to have a bridge placed. For anatomical and financial reasons implants cannot be used either. After root canal treatment the stump of tooth 48 was restored. The right technique of reconstruction needs to be selected. The composite materials cannot be pushed into the gingival attachments. Then the abutment teeth were contour ground. The patient had high aesthetic demands; therefore, an all-ceramic bridge was placed.



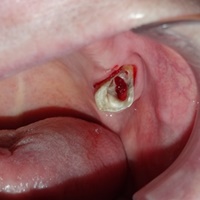
The patient fractured the buccal side of his tooth. The fracture line reached about 3 mm below the gingival attachment. An attempt was made to save the tooth by lengthening the clinical crown. After the surgery, the patient was provided with a temporary prosthetic solution. The final crown was made six months after the surgery.




Proper determining the occlusal plane and the mutual position of dental arches is of paramount importance. Here are the before and after photos of the patient who had her dental arches aligned and their shapes corrected. The difference is visible.


At the age of 89 the patient was in need of some prosthetic treatment. The old crowns were removed. The tooth 26 (top left six) underwent trisection. A complete upper denture was anchored on top of three telescopic crowns. The photos below show the intraoral view before treatment and the condition after four years after completing the treatment.



-
All-ceramic veneers and crowns
The best aesthetic results are obtained using all-ceramic veneers and crowns. Nowadays they are made from porcelain of lower hardness, so that the teeth from the opposing dental arch are less susceptible to damage.




The patient turned up for treatment when the old composite tooth reconstruction fell off. The photo shows obsolete composite restoration solution: a wire manually bent and covered in composite.




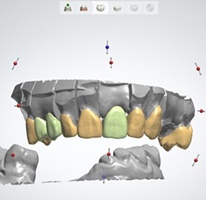
The patient aged 30, comprehensively treated (conservative, orthodontic and prosthetic treatment). On the incisors and canines we can see all-ceramic veneers made by CAD-Cam method. All-ceramic crowns have been placed on the premolars. The patient opted for the lightest shade of teeth (after bleaching).



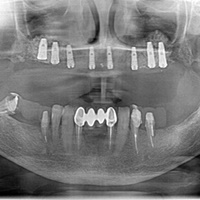
All-ceramic crowns on Branemark bridge. Patient aged 68. Prosthetic work has been done on the whole upper dental arch. The mandibular molars are reconstructed on implants.




Six years ago a reconstruction of the whole upper dental arch was made. It included all-ceramic crowns and bridges. Tooth 22 was rebuilt on an implant. Good hygiene. The condition is stable.
-
Complex prosthetic rehabilitation








Business woman. Stressful lifestyle, non-smoker, bruxism. Wax-up was made, in order to assess the aesthetic a mock-up was made as well. All-ceramic veneers were used at the front and all-ceramic crowns and bridges were used on the sides.







An example of both jaws rehabilitation. A patient with a long history of neglecting dental treatment. Abrasion, spontaneous extrusions, dentoalveolar compensation, broken gum line. It was relatively difficult to rebuild the occlusal plane and the alignment of the gum line. The upper jaw holds all-ceramic crowns and bridges, and skeletal dentures on bolts. The lower jaw features crowns and bridges: porcelain on metal. The end result is satisfactory to the patient.




Large treatment needs. The patient wore upper and lower skeletal dentures. For several years the dentures were not relined nor were they adapted to the changing conditions in the oral cavity. The vertical dimension of occlusion was restored. The aesthetic segment: porcelain on metal, support zone: dentures on latches.
-
Removable dentures, retention elements enhancing the stability of dentures
Various attachments such as latches, clips, magnets, kerators, locators or beams can be used. All of these elements significantly improve the adhesion of removable dentures to a prosthetic base.




The patient aged 42. For 20 years she has had tooth deficiencies in the lateral parts of the mandible and maxilla. For several years she has been suffering from complete edentulism in the maxilla. The patient had removable acrylic gum supported dentures, but could not use it. The front lower teeth were reconstructed with porcelain crowns. The support zones are enhanced by skeleton, fastened with snaps. Complete dentures in the upper jaw.




The patient aged 50, working with her voice. A serious aesthetic and phonetic defect. The patient tried to wear partial acrylic dentures, but without success. The labial section was rebuilt with porcelain crowns and bridges. Skeletal dentures are placed on the sides.




Bilateral deficiencies in the mandibular wing. Strong teeth abrasion of the remaining teeth in the labial part. Lowered height of occlusion. Deficiencies in wing were restored with skeletal dentures on ball attachments. The crowns of lower incisors were rebuilt using onlays, keeping the pulp of all incisors living.




The patient aged 58. For eight years she was using complete lower dentures, supported in the labial part on telescopic zirconium crowns. The condition is stable. Only after 6 years of using the dentures, the need arose to reconstruct keratinized gums on the labial side of the ridge. Every two years, the dentures are relined.




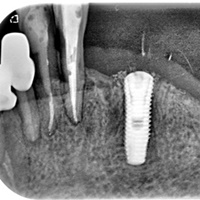


Removable dentures in the maxilla, bridge on telescopes, on the right side rested on a saddle. Skeletal dentures on three telescopic crowns were placed in the mandible. After breaking crown of tooth 33, the root was extracted and an implant with a locator was embedded. The patient has been using the prosthetic replacement for seven years.