




THE HIGHEST QUALITY DENTISTRY

THE HIGHEST QUALITY DENTISTRY

DENTAL IMPLANTOLOGY
Treatment involving intraosseous implants is regarded as a real breakthrough in replacing missing teeth. This method allows, in a manner most similar to the physiological one, to transfer occlusal forces during chewing and reconstruct missing teeth. Initially, implants were placed in areas where after tooth loss a sufficient amount of alveolar bone was preserved. Unfortunately, after tooth loss, loss of alveolar bone and gums covering it, is a physiological process. Hence, attempts were made to adapt the shape and size of intraosseous implants to changing conditions in the oral cavity. With time, doctors have learnt to reconstruct the missing bone tissue and gums, and consequently, we currently know multiple ways to rebuild the missing soft tissue and bone tissue.
According to Dr Marius Steigman, one of the authorities in the current world of implantology, implants should be placed in places with no bones and gums, however, in places which anatomically correspond to the position of our teeth. Only this method guarantees the prosthetic reconstruction which functionally and aesthetically resembles the patient's real teeth. Still, there is one important detail we need to mention. Before placing an implant, there is a need to reconstruct the missing tissue using regeneration treatment. This stage is the biggest challenge for the surgeon and it causes the most problems. Which operating procedure should be chosen? Which bone substitute should be used? Should biomaterials be used? Which membrane should be applied during the guided tissue regeneration? There are many questions and answers. The same situation concerns implantation techniques. Implants may be placed immediately after a tooth extraction, sometimes delayed implant placement is advisable, sometimes the dentist decides to combine placing an implant with rebuilding the missing bone tissue and gums, etc.
There is a large variety of surgical techniques, biomaterials, sewing techniques. Placing an implant is a relatively simple phase of treatment, provided that an appropriate implant has been selected, the right implantation technique has been chosen and the prosthetic superstructure has been used for the right time. Developments in biomaterials production, implants production technologies, and the increasing diversity of implant systems lead us to formulate the following question: Which implant system is the best, which implant system is the most successful in the long run? There is no definite answer, but each implant clinic, for marketing reasons, convinces us that their product is the best, and the use of precisely this product guarantees the biggest satisfaction over the years.
Contrary to online opinions, often going along with advertising practices sponsored by companies offering implant systems, it must be said that in dental implantology, (which is a part of microsurgery) the dentist’s knowledge and experience are of crucial importance. This is a personal opinion of an expert in the world of modern implantology, Fuoad Khoury, who claims that neither the brand of an implant used nor the name of the company producing biomaterials determine the success, but the knowledge and the skillful hands of a dental surgeon.
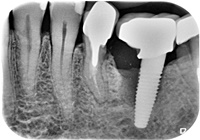
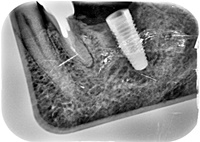

The patient had a "top shelf" implant placed. Unfortunately, a company that for some time was promoting the implant as a real breakthrough in dental implantology, after several years of presence on the market, withdrew the offer. The reason was the large number of complications, periimplantitis. In this case, problems could have been also caused by a carelessly made prosthetic phase. The implant was removed, a new one was placed and the bone was regenerated. The final X-ray was taken two years after the end of treatment.
We offer a variety of implants, according to the conditions in the oral cavity, and the expectations and requirements of our patients. The implant systems used in our clinic have been successfully used by other doctors for many years and are continuously improved by their manufacturers. The Nobel Biocare implant system was first presented in Toronto in 1982 and it has been improved and modified since then. The TBR, Alpha Bio implant systems have been available on the market for about 20 years. The Miss system is a continuation of the Alfpha Bio line. Our patients often decide to use the Korean Dentium Superline implants, available on the Polish market for several years. In my opinion, the Dentium Superline implants guarantee a favorable quality-price ratio. Nevertheless, we are able to place implants made by any producer and belonging to any implant system, according to our patients wishes and previous arrangements.
Currently, there are many different implant systems available. In Poland there are several dozen different implant systems on the market. It is difficult to assess how many implant systems are available in Europe. It is estimated, however, that about 10% of these systems disappears from the market each year, and the same number of new systems appears. Therefore, when choosing an implant system, one should learn for how long it has been accessible. Is the system reliable?
Today, we observe almost exclusive use of implants in the shape of a threaded cylinder or a cone. The various implant systems differ when it comes to technical details. Therefore, it is rather inadvisable or not always possible to connect together components of different implant systems.
A few years ago you could find such a slogan created by one of the major implant manufacturers: "Every dentist offers crowns, bridges, implants ...". If we carefully consider these words, we should sympathize with those patients who believed that surgical and prosthetic treatment using implants, is as simple as filling a cavity or placing a prosthetic crown. Especially when we know that placing a good quality filling or a crown is an art and it is very easy for a dentist to make a mistake. We must therefore distinguish between the real possibilities of implant treatment and advertising tricks.
An important role is played by the experience and knowledge of a doctor, it often happens that the real opportunities are different from those presented in commercials. Another important issue is the relatively high cost of placing implants, which on one hand is often caused by the individual conditions in the patient's mouth, and on the other hand, by their expectations, requirements and… wishes. Therefore, we always present some alternative ways of treatment to our patients within the proper treatment procedures. However, even the highest costs incurred by the patient cannot replace personal hygiene, cooperation with the dentist and regular dental checkups, as well as following the guidelines of the treatment plan. We do recommend that our patients with implants see the dentist at least once a year and have postoperative X-rays taken. For example, in the case of patients without any symptoms and without changes in the tissue around implants, the first checkup X-ray is taken two years after the surgery.
It means placing implants in the bone, immediately after tooth extraction. This solution is relatively attractive to the patient, because it provides the possibility to reduce the total treatment time and helps to minimize loss of bone and gum tissue after tooth extraction. Note, however, that this kind of implant placement is possible only with specific favourable conditions(healthy bone, in the right amount, requirements for soft tissue need to be fulfilled, favourable occlusion conditions, etc.)
With favourable occlusion conditions, a temporary prosthetic superstructure may be immediately placed after extraction. After a few months, one should get a final prosthetic superstructure.
We must therefore consider all treatment options and after an appropriate analysis we may qualify the patient for immediate implant placement, delayed implant placement, or treatment in stages. Most patients require treatment in stages and only some of them may be offered immediate implant placement. It should be noted though, that the immediate implant placement, although desired by patients, is subject to a higher risk than the standard step by step dental implant treatment.
As the name suggests, this technique involves placing implants in the bone without gums incision. Access to the bone is obtained by cutting a circular opening in the gum with a special surgical knife, so it is possible for a bone cutter to prepare the implant bed, and place the implant as the final step. Such implants may be immediately attached to a prosthetic crown or a healing abutment until the end of the prosthetic restoration process. This way of implant placement may be very attractive to the patients, still, this method gives worse results especially when assessing long term aesthetic profile of the soft tissue around the crown attached to the implant. Therefore, it is most frequently used in the side sections of the dental arch.
During the surgery, one may encounter many situations that force the dentist to make changes in the surgical technique, and even refrain from performing implant placement without gums incision. Only a small number of patients are suitable for this type of surgery because certain alveolar bone conditions need to be fulfilled. The biggest disadvantage of the procedure, particularly in the so-called boundary conditions, is the lack of visual inspection of the treatment area.
Immediate implant placement and crown attachment… or “teeth in one day”, is quite a popular slogan encouraging patients to begin treatment. There is only one problem: the number of patients who can safely qualify for this type of treatment is very small. The osseointegration phenomenon, which is the fundamental stage of treatment with the use of dental implants, is a dynamic process which requires certain conditions to be fulfilled. Personally, I rarely attach implants to prosthetic construction immediately after their placement in the bones. Precisely because the requirements for the soft tissue profile, the alveolar bone architecture and the occlusion requirements are fulfilled in the case of a very small number of patients. However, each case should be treated individually and each patient should be qualified for the surgery depending on the local and general conditions.

&
















































